")

News & Information
Stay up-to-date on the latest wellness developments, data and trends from industry thought leaders and expert in the field.
-
 Integrating Sleep Into Your Workplace Wellness Strategy
Integrating Sleep Into Your Workplace Wellness StrategyMay 5, 2025
While we understand its importance, sleep is often the first thing sacrificed when other priorities take over. Today's blog presents common barriers to rest that employees may face, along with suggestions for how to address them effectively.
-
 The Well Workplace Process Explained
The Well Workplace Process ExplainedApril 28, 2025
The Well Workplace Process demonstrates an organization's commitment to creating a supportive, healthy workplace while also fostering employee well-being and long-term organizational success.
-
 Celebrating Earth Day: Highlighting Social Wellness and Sustainability in the Workplace
Celebrating Earth Day: Highlighting Social Wellness and Sustainability in the WorkplaceApril 21, 2025
Organizations can make a positive impact this Earth Day and beyond by supporting employee well-being, enhancing workplace wellness initiatives, and improving our planet through thoughtfully integrated wellness initiatives.
-
 Helping Employees Cope With Stress Without Turning to Alcohol
Helping Employees Cope With Stress Without Turning to AlcoholApril 14, 2025
Given the widespread use of alcohol, it's nearly impossible to ignore the physical and mental impacts of using these substances as a coping mechanism. Creating an inclusive environment that helps employees discover healthy alternatives for managing stress can make a significant difference.
-
 Building a Psychologically Safe Workplace: A Key Step in Reducing Employee Stress
Building a Psychologically Safe Workplace: A Key Step in Reducing Employee StressApril 7, 2025
The Occupational Safety and Health Administration (OSHA) reports that 80% of U.S. workers experience stress. Employers can support employees with stress management by fostering psychologically safe workplace environments.
-
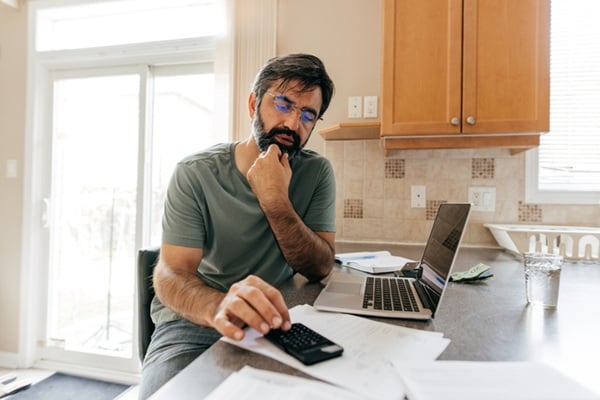 The Real Savings of Financial Wellness
The Real Savings of Financial WellnessMarch 31, 2025
Financial stress can negatively affect both physical and mental health. When financial stress is reduced, employees report being happier and more engaged. A workplace well-being strategy that includes financial wellness initiatives can deliver long-term savings for employees and employers.
-
 Water, Wellness, and the Workplace: How Water Impacts Employee Health and Productivity
Water, Wellness, and the Workplace: How Water Impacts Employee Health and ProductivityMarch 24, 2025
While the warmer months often bring hydration to the forefront of our minds, National Nutrition Month offers another important reminder to prioritize fluid intake year-round.
-
 Food Culture in the Workplace
Food Culture in the WorkplaceMarch 17, 2025
March is National Nutrition Month—a time to reflect on the importance of healthy eating and recognize the barriers that can make it challenging.
-
 Continuing Education and Work–Life Harmony
Continuing Education and Work–Life HarmonyMarch 10, 2025
Maintaining balance and work–life harmony can be challenging when faced with increased responsibilities on top of regular work tasks and home–life roles, but supportive employers can make a difference. Learn key strategies to support employees pursuing continuing education opportunities in today's blog.
-
 Empowering Women by Supporting Their Well-Being at Work
Empowering Women by Supporting Their Well-Being at WorkMarch 6, 2025
Nearly 77% of women are currently in the workforce, and supporting their well-being at work is a necessary step toward achieving gender equality. By recognizing the complexities they face, employers can implement targeted strategies to empower women in the workplace.
Categories
- Belonging (3)
- Benchmarks (3)
- Benefits (4)
- Cancer (2)
- Culture (16)
- Emotional Wellness (14)
- Healthy Workplaces (13)
- Intellectual Wellness (14)
- Legal and Compliance (6)
- Mental Health (8)
- Occupational Wellness (11)
- Physical Wellness (14)
- Social Wellness (9)
- Spiritual Wellness (3)
- Wellness Alliance Events (1)
- Wellness Initiatives (12)
- Workplace Wellness (5)